pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Jeongwu Seong,Yeona Kim,Jungsoo Lee,Kihyuk Shin,Hoon-soo Kim,Byungsoo Kim,Moon-Bum Kim,Hyun-Chang Ko
10.17966/JMI.2026.31.1.48 Epub 2026 March 31
Abstract
Keywords
Cryptococcus neoformans Immunocompetent Primary cutaneous cryptococcosis Ulcer
Cryptococcosis is a systemic fungal infection caused by Cryptococcus species, with inhalation as the primary route of entry. It can disseminate hematogenously to several organs, including the central nervous system and skin. Cutaneous lesions are usually secondary, occurring in 10-20% of dis- seminated cases1. Primary cutaneous cryptococcosis (PCC), resulting from direct inoculation is rare and typically occurs in immunocompromised hosts, although a few cases have been reported in otherwise healthy individuals2,3.
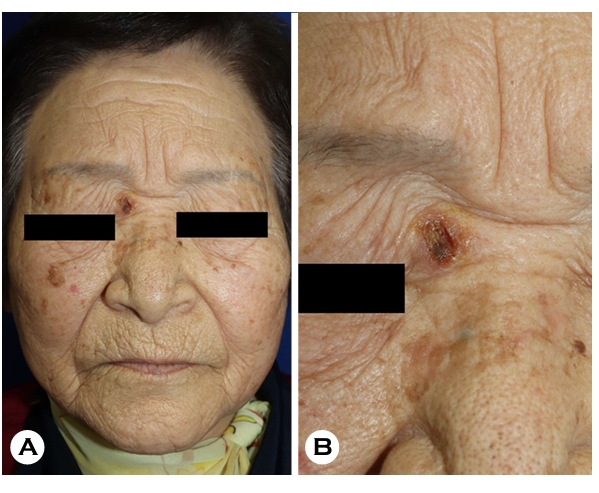
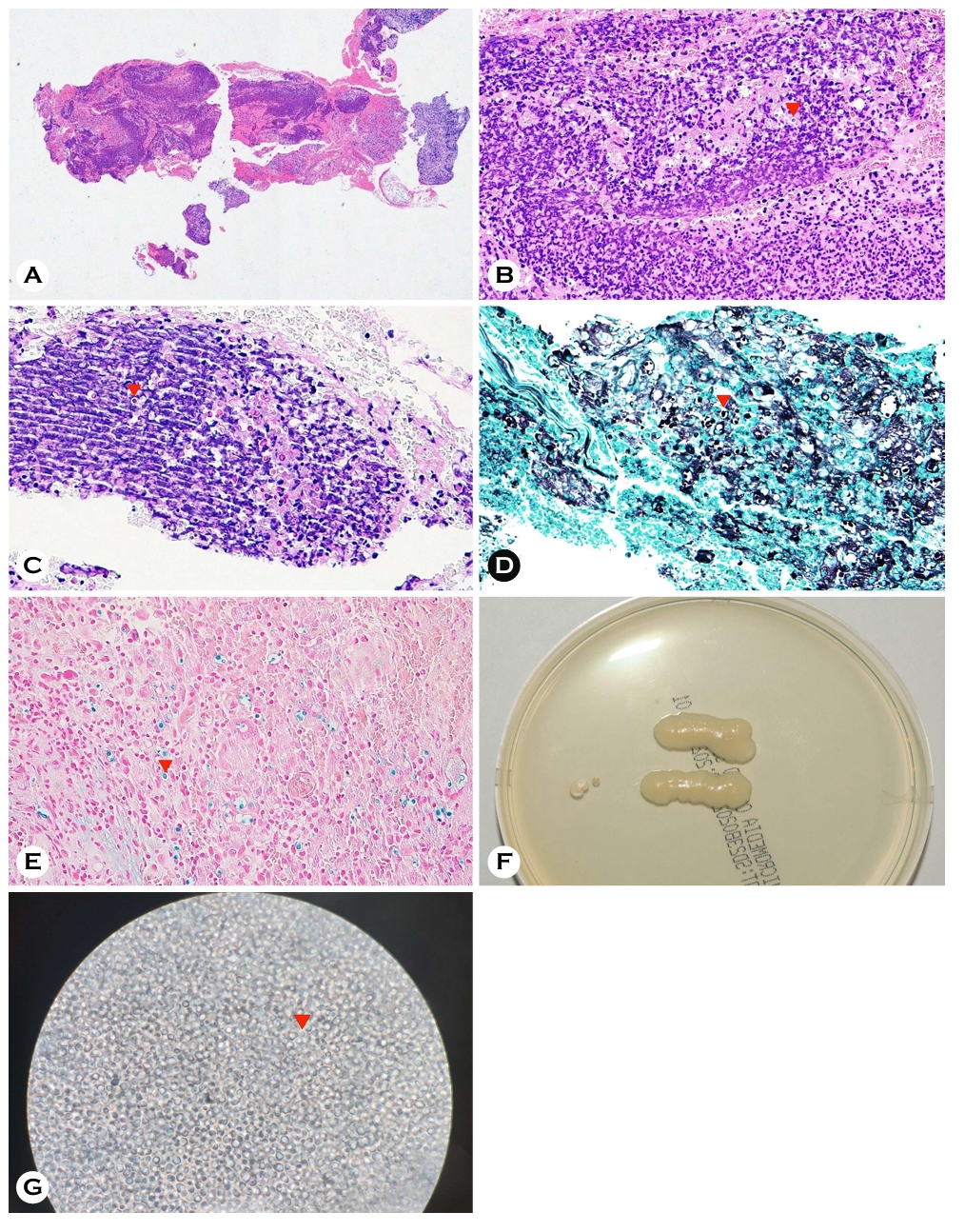
An 84-year-old woman presented with an ulcer in the right inner canthal area (Fig. 1A, B), which was associated with mild pain, tenderness, and pruritus but no systemic symptoms. The lesion had been present for 4 months, and no prior treatment had been administered. The patient had no history of diabetes mellitus, malignancy, chronic kidney disease, or HIV infection and had not taken immunosuppressive medications. She also reported no exposure to pigeons/avian excreta, other animals, or recent travel. Histopathology showed dermal inflammatory infiltration with numerous round yeast spores (Fig. 2A, B), and special stains highlighted encapsulated yeast (Fig. 2C-E). Tissue culture yielded creamy mucoid colonies (Fig. 2F), and lactophenol cotton blue staining demonstrated yeast cells with a capsule-like halo (Fig. 2G). 18S rRNA gene sequencing confirmed Cryptococcus neoformans. Serum cryptococcal antigen and HIV tests were negative. Computed tomography of the brain, chest, and abdomen along with cerebrospinal fluid analysis, showed no evidence of systemic involvement.
The diagnosis of PCC was established according to the Noble and Fajardo criteria (absence of systemic infection, identification of C. neoformans from the skin lesion, and no extracutaneous involvement within the preceding 4 weeks). The patient was treated with oral fluconazole (6 mg/kg once daily). After 1 month, the lesion showed marked improve- ment, leaving only mild scar-like changes.
PCC shows polymorphic, nonspecific cutaneous manifest- ations, including nodules, ulcers, and cellulitis- or whitlow-like lesions, and may mimic other dermatologic conditions, including basal cell carcinoma (BCC)2,4. However, cutaneous cryptococcosis mimicking BCC has been reported mainly in immunocompromised hosts, suggesting that host immune status may influence the clinical morphology of cutaneous cryptococcosis. Our case is notable for a similar presentation occurred in an immunocompetent patient. Although some case-based reviews have suggested favorable outcomes with itraconazole, our patient responded well to oral fluconazole, supporting its use in selected cases2.
Although PCC has been frequently described in immuno- compromised hosts, it is increasingly recognized that the disease can also occur in immunocompetent individuals3. In previously reported Korean cases, PCC was often associated with comorbidities, corticosteroid exposure, or local predis- posing factors such as trauma5, whereas our patient had no identifiable risk factors. While the precise route of infection remains unclear, inoculation through minor unrecognized skin breaks cannot be ruled out2.
This case is clinically meaningful because PCC presented as a solitary ulcerative facial lesion mimicking BCC in an immunocompetent elderly patient. Therefore, when a chronic ulcerative lesion develops on the face and follows an atypical course, PCC should be included in the differential diagnosis, and definitive diagnosis may require histopathological exam- ination with adjunctive mycological studies.
References
1. Noble RC, Fajardo LF. Primary cutaneous cryptococcosis: Review and morphologic study. Am J Clin Pathol 1972; 57:13-22
Google Scholar
2. Neuville S, Dromer F, Morin O, Dupont B, Ronin O, Lortholary O. Primary cutaneous cryptococcosis: A distinct clinical entity. Clin Infect Dis 2003;36:337-347
Google Scholar
3. Gaviria Morales E, Guidi M, Peterka T, Rabufetti A, Blum R, Mainetti C. Primary cutaneous cryptococcosis due to Cryptococcus neoformans in an immunocompetent host treated with itraconazole and drainage: Case report and review of the literature. Case Rep Dermatol 2021;13:89-97
Google Scholar
4. Silva Souza CD, Takada MH, Ambiel MV, Nakai VT. Primary cutaneous cryptococcosis: The importance of early diagnosis. An Bras Dermatol 2021;96:482-484
Google Scholar
5. Kim TW, Park SM, Moon JH, Song M, Kim HS, Kim BS, et al. Primary cutaneous cryptococcosis in a patient with pulmonary tuberculosis. Korean J Med Mycol 2013;18: 111-116
Google Scholar
Congratulatory MessageClick here!